Suicide is the intentional taking of one's own life. Many believe that when a teenager commits suicide is it not only the waste of a life, but also a nullification of potential. Statistics show that 11.4 in 100, 000 youths (15-24 years old) commit suicide. It is the third leading cause of death in this age group. The rate increased from 4.0 in 1956 to 11.4 in 1997 (McIntosh 1999). These statistics are frightening. When a teenager commits suicide those left behind are in emotional pain. The family, the friends, the school, the church, the neighbors and even people who learn about it feel the pain in varying degrees (Gardner 1985; Schneidman 1970). The two questions usually asked are: Why did this happen and what could have been done to prevent this tragedy? The experts in suicidology, mental health and education agree that the absolute key to prevention is education. What they do not agree upon is how to effectively measure if suicide prevention programs are actually reducing youth suicides.
There are thousands of youth suicide prevention programs being conducted throughout the world. These prevention programs are proposed plans to keep youth from intentionally taking their own lives. A basic assumption determined by the literature review is that the best places to introduce prevention programs are in the schools (Smith 1986). Children are required by law to attend school and thus they are a captive audience. One such program, the Yellow Ribbon Program, was introduced into the South Bend Community School Corporation through the efforts of the Community Resource Center (CRC) of St. Joseph County, Indiana. The CRC is a non-profit organization that services the needs of St. Joseph County through two telephone services. The Helpline is dedicated to helping people with problem assessment information and referrals. The Crisis/Suicide Intervention Hotline is a 24-hour, seven day per week volunteer based service for people in crisis.
A presentation by the CRC was made at the Century Center in South Bend, Indiana, in October of 1999. The group consisted of school personnel, students, parents and interested members of the community. The Yellow Ribbon Program is a campaign dedicated to the prevention and awareness of youth suicide. It is a vehicle through which the Light for Life Foundation International reaches out to teenagers all over the globe in hopes of preventing youth suicide. The Foundation was started in September of 1994 by the parents of Mike Emme, a seventeen-year old male who committed suicide by shooting himself (Light for Life 1995-1999). The Program emphasizes awareness and prevention of teenage suicide. It revolves around a little yellow card that gives a student the opportunity to reach out for help. Programs similar to this are usually brought into a school system by an outside organization dedicated to assisting in suicide prevention (US Department of Health et al. 1992; Capuzzi 1988); this is the case regarding the presentation of the Yellow Ribbon Program by the CRC.
The purpose of this research project is to determine if the Yellow Ribbon Program made a measurable impact on the urban school community where it was introduced to. Impact is defined in this context as the changing of students' knowledge of suicide; an increase in their contacts with school social workers pertaining to suicide; an increase in calls to the CRC Crisis Hotline pertaining to youth suicide; if the support to the CRC from outside sources for the Program changed; and/or a change in any existing school program that promotes students' not committing suicide. This research was conducted in a non-experimental framework (non-laboratory controlled) and within the emancipatory paradigm. Emancipatory within this framework is defined as: willingness by the researcher to be open and willing to change procedures and methods as the project progresses if deemed necessary to the overall good of the participants and the recipients.
METHOD
Participants
A director of a community based organization (the CRC) and four social workers (all possessing a Master's degree in Social Work) from an urban school corporation (SBCSC) were the participants in this research project. The director of the CRC was chosen because she was the head of the organization that did the presentation and her knowledge of the procedure for that presentation was extensive. The social workers were chosen because they are the people who have the documented contact information with the students as it relates to suicide. These small samples were chosen due to availability and the knowledge level of the participants. Each one was initially contacted by telephone and given an overview of the project. Consent was obtained from the employer of the social workers' boss before contacting them. All agreed at the time of the telephone call to participate. No compensation was given for their participation. Each participant signed a consent form that was in agreement with the standards set forth by the Institutional Review Board of Indiana University South Bend.
Materials
Two different questionnaires were used in this study: one for the director, and one for the social workers. (Refer to Appendix A and B for copies of the questionnaires). The thirteenth question of each was the interview section. The first eleven questions of each were qualitative in nature and were coded on a Likert scale. The range was: 5 = excellent, 4 = above average, 3 = average, 2 = below average and 1 = poor. The first five questions were the same on each questionnaire. These questions pertained to the participant's perception of the Yellow Ribbon Program. The next six questions were relevant to each setting (see Appendix A and B for specific questions). The 12th question was quantitative and requested the number of calls to the Hotline before and after the Yellow Ribbon Program was presented. The measurement was determined by the number of contacts with the social workers or phone calls to the CRC's telephone hotline. The 13th question was the interview and was tape-recorded. Each participant gave prior consent for this procedure. The interview was coded by six keywords: networking, communication, evaluation, goals, future intent and benchmarking. These six words were chosen from an analysis of the literature review (Here for Life 1996-2000).
Procedure
The processes of filling out the questionnaires and giving the interviews were conducted in each participant's office. The date (in the last half of March, 2000) and time had been agreed upon previously between each participant and the researcher. Each participant was given as much time as needed to fill out the questionnaire. Restating to each participant the 13th question started the interview. That question states, "Are there any other comments, ideas or pertinent information that you believe should be addressed in this interview?" The participant was given all the time they needed to give their opinions, feelings and statements. If in this unstructured part of the interview they did not address any of the six keywords, the interviewer would then prompt the interviewee with those words. After addressing those keywords the procedure was then complete.
RESULTS
The results of the interviews with the social workers, using the six keywords, are as follows: networking was only done on a local basis; communication (within the school environment) was mainly done only when crisis situations happened; evaluation was done in the context of other implicators (see discussion); goals and future intent were to continue suicide prevention (not specifically Yellow Ribbon); benchmarking was none that they knew of. The results of the averages (the mean, M) for the first eleven coded questions are graphed in Figure 1.
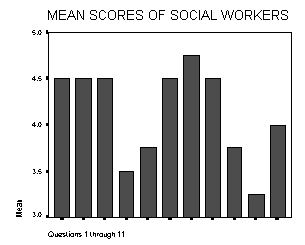
Figure 1: Mean (M) scores of social workers of questions 1 through 11.
The CRC director interview results were: networking there was one local contact, one out of state contact and a few internet sites; communication (with the schools) was strong for introduction of the program and little since; evaluation was done by their own set of standards; goals and future intent were to continue Yellow Ribbon presentations (dollar constraints); benchmarking was a hope to be the benchmark(of the industry). No mean (M)was obtained for each coded question, because she was only one person. The director's answers for questions 1 through 11 are as follows:
Director's Answers from Questionnaire #1
| Question Number | Ranking |
|---|
| 1 | 3 |
| 2 | 5 |
| 3 | 5 |
| 4 | 4 |
| 5 | 5 |
| 6 | 4 |
| 7 | 4 |
| 8 | 3 |
| 9 | 4 |
| 10 | 5 |
| 11 | 1 |
The mean (M) scores from the social workers and the scores the director gave for the questions are intended to be a benchmark for further analysis of prevention programs in their settings.
There was no significance (two tailed) obtained between the number of contacts (per month) to social workers before and after their presentations in their specific schools. This was calculated by using a paired samples t-test. The results are (t(3) = -1.414, p = 0.252). The p value must be < 0.05 to be significant. What this statistic says in layman's terms is that the number of contacts to social workers before and after the presentations did not change enough to attribute that change to the presentation. The CRC had zero calls the month before the presentation was made to school personnel and fifteen the following month. This cannot be calculated to significance because of the amount of unidentified extraneous variables that could have been present that warranted those fifteen calls. Possible examples of those variables: advertisement of the Hotline by the CRC, suicide education not related to the Yellow Ribbon Program, personal decisions to call the Hotline not based on the Program, prank calls to the Hotline, or errors in documentation of suicide calls.
DISCUSSION
One fact came to light in each interview about the Yellow Ribbon Program. The cards seem to have the greatest impact with the students. They use them, they talk about them and they ask for them. The Community Resource Center and the South Bend Community School Corporation demonstrate the same techniques in suicide prevention as the rest of the nation. They know it is an immense problem; they are dedicated to the problem and yet they are operating and evaluating mostly in their own settings. This is transpiring because there are no standards to judge the Program's progress, success or impact.
Time and money are the keys to the success of measuring suicide prevention; time for the schools and organizations to do evaluations and money from greater sources than just the efforts of those community based organizations. Without standardized evaluations, improvement is at a great risk of never transpiring. The CRC will only continue to do presentations if the monies are available. They do not have the means or the resources to conduct a systematic evaluation. This takes personnel, time and dollars beyond their grasp. This community, like others, must measure suicide prevention against their own standards because there are no industry standards, only suggestions (Berman 1995). The absence of ongoing networking is another contributor to the lack of systematic standards for measuring impact (Zenere 1997). A gap in communication exists due to time constraints. For example, one social worker stated, "When you are responsible for 2,200 students, all you do is put out fires." Each social worker stated that suicide prevention is only a part of a much greater over all picture. This was made clear in the literature review. The overall picture involves drug awareness, reductions in teen pregnancies, decreased drop-out rates, increased peer facilitation groups, life skills training, self-esteem building techniques and countless others (Here for Life 1996-2000). This big picture is part of the answer to the question, "What could have been done to prevent this tragedy?" Suicide prevention exists inside other programs. It needs to start early in a child's school career and be an ongoing process until graduation.
The problems encountered in this research project were many. The lack of quantity in each sample was limited and this made statistical analysis difficult. The significant statistic is in question due to small sample size. Validity and reliability are most likely in question. Validity is in question because measuring impact was rendered difficult by the possibility of extraneous variables. Reliability would be difficult due to the uniqueness of the interviews and the researcher's choice of keyword coding. The coding was based on the literature review but it was limited in content and context due to a lack of previous research. The lack of systematic procedures for evaluating suicide prevention was an obstacle. This researcher had limited guidelines to know if the procedures and methods were correct. It left this writer trying to answer who, where, how and why questions with little criteria. Researcher bias was a problem; after countless hours in literature review it was difficult to not lead the participants in the interview process. This of course could have had an impact on the results due to the possibility that the interviewees may have answered differently without the bias.
Did the question, "Did this study measure the impact of a youth suicide prevention program?" get answered? The answer would have to be no. Did this suicide prevention program prevent a youth from committing suicide? The answer is unknown. What this study did accomplish was to bring to light a process that needs improving. This coincides with the literature review (Berman 1995; Capuzzi 1988; US Department of Health et al. 1992; Zenere 1997). This improvement cannot, and will not, be accomplished until this nation (and the world) dedicates its time, energy and money into saving its greatest resource, its children.
RECOMMENDATION
The results of this project brought forth a glaringly apparent fact: the Community Resource Center and the social workers of the South Bend Community School Corporation are very dedicated to teenage suicide prevention and awareness. In all five interviews the emotional content was present in each person. The question now arises as to how these five dedicated and caring people can most effectively increase awareness and prevention in the area of teenage suicide.
One recommendation is for all the participants in this study to meet and discuss their perceptions of the Yellow Ribbon Program, their perceptions of each other and what each one has learned in the process of presenting the Yellow Ribbon Program. This is a direct line of communication that will hopefully look at the presentation, implementation, feedback and the problems encountered. With this information, the needs of the social workers and the CRC could be addressed. This is a recommendation that comes from the simple ideas of teamwork.
The second recommendation is for a new, specific, systematic and concentrated program to be created for and maybe even with the parents. Parental participation seems to be one aspect that must increase (Here for Life 1996-2000). Each interviewee indicated that if education and awareness began in the home, the fight against teenage suicide would have an additional ally. Early intervention is one key to preventing suicide. This intervention needs to occur as early as when a child acts out, or shows signs of depression, or gets in trouble with the law (Zenere 1997). The wall of denial must be brought down. Parents need to have a heightened awareness of the problems and each interviewee stated this with emphasis. This program would require the efforts of the South Bend Community School Corporation and the CRC. Awareness is the key to preventing problems down the road. The phrase "forewarned is forearmed" applies to this situation.
The lack of networking is a global problem as it pertains to teenage suicide. Communities all over the world are attempting to help their at-risk children. The problem is that the implementers and providers are mostly communicating locally and, on occasion, regionally. They communicate with each other and with other local community agencies (Capuzzi 1988). This is also true of the participants in this project. Each one admitted in the interview that their networking was lacking in context and content. The third recommendation is that participants need to broaden the scope of their network. The change from a micro to a macro network needs to transpire. This change will not only increase the knowledge of prevention programs that are successful but also those that are not successful (Capuzzi 1988; Here for Life 1996-2000; US Department of Health et al. 1992; Zenere 1997). It would give greater insight into the methods and resources that others are using. Each community, South Bend included, runs and evaluates itself in its own reality. The "re-invention of the wheel" appears to occur almost every time a suicide prevention program is introduced (US Department of Health et al. 1992). This is a considerable waste of time and money. If broader (hopefully global) networking were to occur, the learning process would be shorter, money and time could be saved and ultimately the at-risk children would benefit. This recommendation is supported by the literature review.
The rate of teenage suicide has tripled since 1956 (McIntosh, 1999). This statistic is significant by any type of measurement. The findings of the literature review found no organization that specifically addresses the problem of evaluating teenage suicide prevention programs. There are no systematic standards for evaluation of suicide prevention programs (Capuzzi 1988; US Department of Health et al. 1992; Zenere 1997). The obvious situation that this causes is one that goes to the core of the problem. If no valid and reliable evaluations are being done then how are the improvements to occur? The problem also asks, "How does a community know if they are doing what is best for the children?" The last recommendation transpires from this problem and is likely the most difficult. The funding for a nationwide organization of this magnitude must come from greater resources than are available in the local communities (Here for Life 1996-2000). Educators, mental health workers, parents and all who are dedicated to the youth of this nation must come together and fight for our children. This fight should come in the form of organized groups contacting our local, state and national governments to obtain funding and support for these programs. These groups need to also contact the media over and over until someone listens and takes action.
"United we stand, divided we fall," applies to the prevention of teenage suicide. We must preserve and protect our children for they are the future and the hope of this nation and the world.
APPENDIX A
Questionnaire #1
(To be given to the Director of the Community Resource Center of St. Joseph County.)
This questionnaire is being given to you as a participant in the study entitled, "Measuring the Impact of Youth Suicide Prevention Program." The program that is specifically being scrutinized is the Yellow Ribbon Program.
Each question, except the last two, will be ranked according to the following criteria: 5 = excellent, 4 = above average, 3 = average, 2 = below average, and 1 = poor. Please circle your answer with care and thoughtfulness, as your answers are quite important.
Thank you for participating.
1. When you first learned about the Yellow Ribbon Program, to what degree did you think the goals of the program were presented?
2. To what degree do you think the Yellow Ribbon Program is dedicated to youth suicide prevention?
3. To what degree do you find the Yellow Ribbon Program relevant to your setting?
4. To what degree do you find the Yellow Ribbon Program's ease of implementing?
5. To what degree do you think the Yellow Ribbon Program will continue to be supported in your setting?
6. To what degree do you think the South Bend Community School Corporation is attracted to the Yellow Ribbon Program?
7. To what degree do you think the presentation of the Yellow Ribbon Program to the South Bend Community School Corporation was received as a viable vehicle to preventing suicide?
8. To what degree do you think you will continue to receive funding for the Yellow Ribbon Program?
9. To what degree do you think solicitation for funding for the Yellow Ribbon Program has the chance to increase benefactors?
10. What has been the response from the business sector for contributions to the Yellow Ribbon Program?
11. What has been the response from the private sector for contributions to the Yellow Ribbon Program?
12. Did the number of calls to the Hotline, pertaining to youth suicide, increase after the presentation of the Yellow Ribbon Program to the South Bend School Corporation?
Average number of calls, pertaining to youth suicide, per month before __________
Average number of calls, pertaining to youth suicide, per month after __________
13. Are there any other comments, ideas or pertinent information that you believe should be addressed in this interview?
This is a verbal response to the investigator. The investigator invites you to be specific in your comments so that a clear understanding of your point of view can be learned.
Thank you for participating in this study.
APPENDIX B
Questionnaire #2
(To be given to four social workers in the South Bend Community School Corporation.)
This questionnaire is being given to you as a participant in the study entitled, "Measuring the Impact of Youth Suicide Prevention Program." The program that is specifically being scrutinized is the Yellow Ribbon Program.
Each question, except the last two, will be ranked according to the following criteria: 5 = excellent, 4 = above average, 3 = average, 2 = below average, and 1 = poor. Please circle your answer with care and thoughtfulness, as your answers are quite important.
Thank you for participating.
1. When you first learned about the Yellow Ribbon Program, to what degree did you think the goals of the program were presented?
2. To what degree do you think the Yellow Ribbon Program is dedicated to youth suicide prevention?
3. To what degree do you find the Yellow Ribbon Program relevant to your setting?
4. To what degree do you find the Yellow Ribbon Program's ease of implementing?
5. To what degree do you think the Yellow Ribbon Program will continue to be supported in your setting?
6. To what degree do you think the Community Resource Center is dedicated to the Yellow Ribbon Program?
7. To what degree do you think the presentation of the Yellow Ribbon Program by the Community Resource Center was well planned?
8. To what degree do you think the presenter possessed expertise in the field of suicide prevention?
9. To what degree do you think the Yellow Ribbon Program has helped educated your students in the prevention of youth suicide?
11. To what degree do you think the Yellow Ribbon Program has helped to educate you in the prevention of youth suicide?
12. Did the number of contacts from students pertaining to suicide increase after the presentation of the Yellow Ribbon Program?
Average contacts per month before the presentation _______
Average contacts per month after the presentation _________
13. Are there any other comments, ideas or pertinent information that you believe should be addressed in this interview?
This is a verbal response to the investigator. The investigator invites you to be specific in your comments so that a clear understanding of your point of view can be learned.
Thank you for participating in this study.
Berman, A., & Jobes, D. (1995) IV. "A Population Perspective, 11 Suicide Prevention in Adolescents (Age12-18)." Suicide and Life Threatening Behavior, 25, 143-154.
Capuzzi, D., & Golden, L. (1988). Preventing Adolescent Suicide. Muncie, IN: Accelorated Development, Inc.
Gardner, S., & Rosenberg, G. (1985). Teenage Suicide. New York: Julian Messner
Here for Life. (1996-2000). [Internet] Available: Hostname:info@hereforlife.org.au
Light for Life Foundation International. (1995-1999). Yellow Ribbon Program. Westminster, CO: Light for Life Foundation International.
McIntosh, J. (1999). Suicide and Depression Class, Spring Semester 1999, Indiana University, South Bend, IN
Schneidman, E. (1970). Recent Developments in Suicide Prevention. In E. S.
Shneidman, N.L. Farberow, & R.E. Litman, (Eds.) The psychology of suicide. p.145-155. New York: Aronson
Smith, J., (1986). Coping With Suicide. New York: Rosen
"US Department of Health & Human Services, Public Health Service, Centers for Disease Control, National Center for Injury Prevention and Control." (1992). Youth Suicide Prevention Programs: A Resource Guide. [Internet] Available: Hostname: aepo-xdv-www.epo.cdc.gov
Zenere, F. III, & Lazaraus, P., (1997) "The Decline of Youth Suicidal Behavior in an Urban, Mulicultural Public School system Following the Introduction of a Suicide Prevention and Intervention Program." Suicide and Life Threatening Behavior, 28. 387-400.


